Ebola Is Once Again a Global Health Emergency
The world is facing the threat of Ebola again. On 15 May 2026, the Ministry of Health of the Democratic Republic of the Congo (DRC) officially declared the country’s 17th Ebola outbreak after laboratories confirmed Bundibugyo virus disease (BVD). That same day, Uganda also reported an imported case from the DRC.
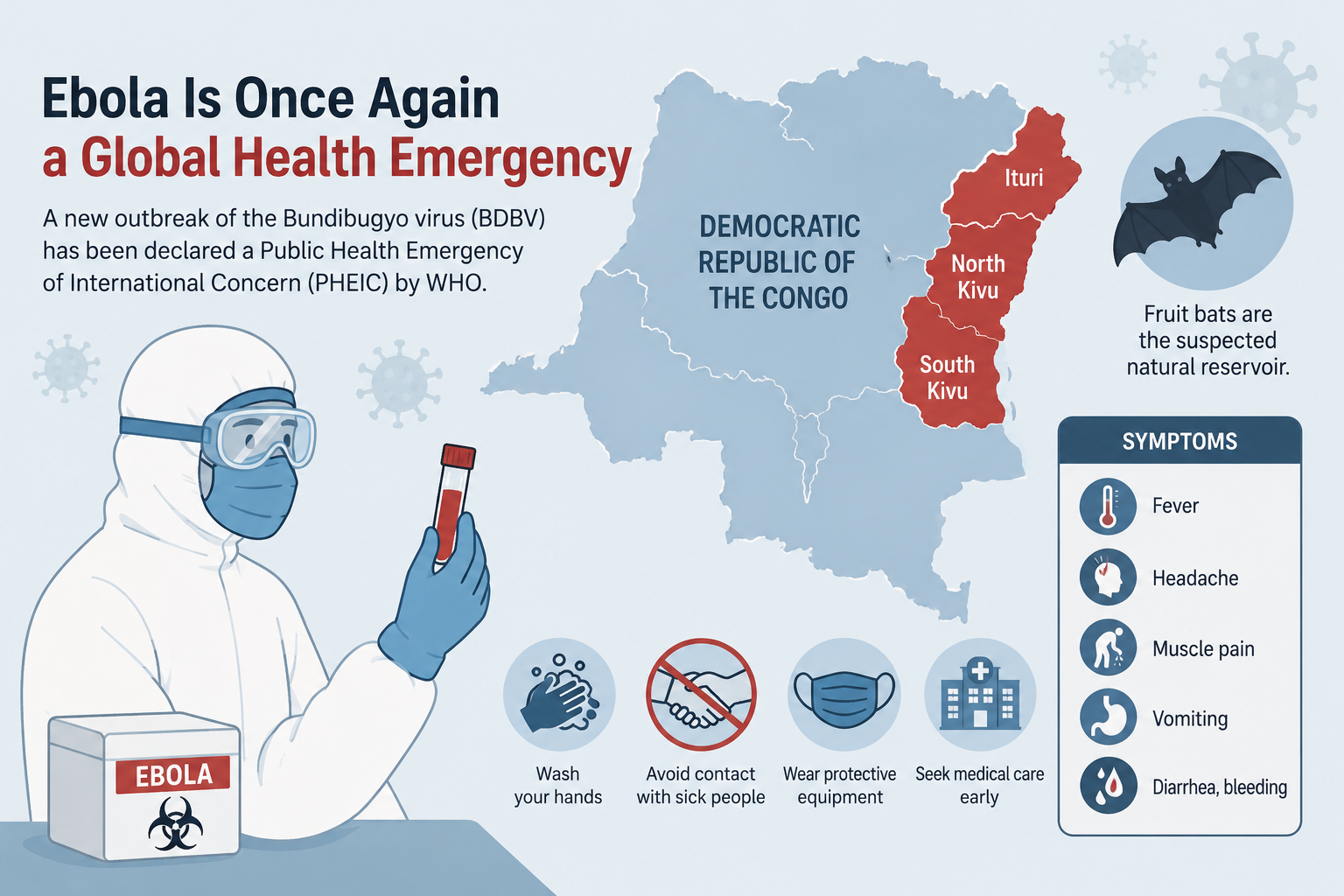
Just one day later, on 16 May 2026, the Director-General of the World Health Organization (WHO) declared the outbreak a Public Health Emergency of International Concern (PHEIC), The highest level of alert the WHO can issue under the International Health Regulations (IHR).
What makes this outbreak different, and more concerning, is the cause: it is not the “usual” strain of Ebola. This article breaks down what the Bundibugyo virus is, why it is far harder to contain than previous Ebola outbreaks, the symptoms to watch for, and how high the risk is beyond the affected region.
Current Situation: Rapid Spread in Eastern Congo
Official WHO data as of 21 May 2026 shows an outbreak growing at alarming speed in the DRC:
- 746 suspected cases with 176 deaths among suspected cases.
- 85 confirmed cases (two of them in Uganda), with 10 confirmed deaths.
- The case fatality rate (CFR) among confirmed cases was around 12%, while previous BVD outbreaks (in 2007 and 2012) recorded a CFR between 30% and 50%.
These figures keep moving. Independent tracking recorded a sharp escalation to more than 1,200 suspected and confirmed cases and over 240 deaths by the end of May 2026. Experts believe the true number of infections could be considerably higher than reported.
Note: Case numbers in an active outbreak change almost daily. For the latest data, always refer to the WHO Disease Outbreak News, which is updated every Thursday.
Transmission is concentrated in three provinces in eastern Congo: Ituri, North Kivu, and South Kivu. The outbreak is believed to have started in the Mongbwalu health zone — a high-traffic mining area — before spreading to Rwampara and Bunia as patients sought medical care.
One of the clearest danger signals: four health workers died within a four-day span at a referral hospital in Mongbwalu, pointing to serious breaches in infection prevention protocols. An American national working as a surgeon in the DRC was also infected and evacuated to a high-level isolation unit in Berlin, Germany.
What Is the Bundibugyo Virus, and How Is It Different?
Ebola is not a single virus. It is a group of viruses in the genus Orthoebolavirus, and several species can infect humans. The best known — and the one most often responsible for large outbreaks — is the Zaire ebolavirus.
The Bundibugyo virus (BDBV) is a different species. It was first identified in western Uganda in 2007, and the 2026 outbreak is only the third time BDBV has been identified as the cause of an outbreak. Like other ebolaviruses, it is a zoonotic disease: fruit bats are suspected to be the natural reservoir, and humans become infected through contact with infected wildlife before the virus spreads from person to person.
Why Is This Strain Harder to Contain?
This is the heart of what worries global health experts. Several factors make the 2026 Bundibugyo outbreak far more challenging:
1. There is no approved vaccine or treatment
For the Zaire ebolavirus, the world already has a licensed vaccine (such as rVSV-ZEBOV) and antibody therapies proven to sharply reduce mortality. For the Bundibugyo virus, there is no approved vaccine or specific treatment at all. Control relies entirely on supportive care, early detection, isolation, contact tracing, and safe burials.
2. Standard rapid tests cannot detect it
The WHO specifically warned that the GeneXpert platform — the rapid diagnostic tool commonly used for Ebola — cannot detect the Bundibugyo virus. This slows case confirmation and makes a rapid field response more difficult.
3. Early symptoms are easily mistaken for other illnesses
The early symptoms of BVD are highly non-specific and resemble malaria, influenza, or fevers caused by the arboviruses common in the region. As a result, there was a detection gap of roughly four weeks between the onset of symptoms in the presumed first case (around 25 April 2026) and laboratory confirmation. During that gap, the virus spread undetected.
4. Conflict and a humanitarian crisis at the outbreak site
Ituri province is gripped by armed conflict, with hundreds of thousands of internally displaced people. This limits the movement of surveillance teams, hampers the transport of laboratory samples, and makes contact tracing extremely difficult — the contact follow-up rate was only around 21%. Combined with Ituri’s role as a commercial and migration hub bordering Uganda and South Sudan, the risk of cross-border spread is high.
Bundibugyo Ebola Symptoms to Watch For
The incubation period for BVD ranges from 2 to 21 days. It is important to understand that a person is generally not infectious before symptoms appear. The progression of symptoms:
Early symptoms (non-specific):
- Fever
- Extreme fatigue
- Muscle pain
- Headache
- Sore throat
Later symptoms:
- Gastrointestinal symptoms (nausea, vomiting, diarrhea)
- Organ dysfunction
- In some cases, bleeding (hemorrhagic manifestations)
Because the early symptoms mimic other febrile illnesses, a definitive diagnosis can only be made through laboratory testing such as PCR or antigen/antibody assays.
How Does Ebola Spread?
The Ebola virus does not spread through the air like COVID-19 or influenza. Person-to-person transmission occurs through:
- Direct contact with the blood, secretions, organs, or other bodily fluids of an infected person (whether living or deceased).
- Contact with surfaces or objects contaminated with an infected person’s bodily fluids.
Transmission is most amplified in healthcare settings when infection prevention protocols are weak, and during unsafe burial practices that involve direct contact with the body. This is why the deaths of four health workers in Mongbwalu were such a major alarm.
How High Is the Risk Outside the Region?
This is the most relevant question for readers far from the affected area. The good news: the current global risk is considered low.
The WHO assessed the risk of the outbreak as very high at the national level in the DRC, high at the regional level in Africa, but low at the global level. The European Centre for Disease Prevention and Control (ECDC) even rated the risk to people in Europe as very low, because transmission requires direct contact with the bodily fluids of a symptomatic patient — not airborne spread.
It is also worth noting that the WHO does not recommend border closures, travel bans, or trade restrictions with affected countries.
Even so, for countries outside the region, the WHO advises basic preparedness:
- The capacity to detect, assess, and manage travelers arriving from affected areas who have an unexplained fever.
- Informing incoming travelers to seek medical attention immediately if compatible symptoms appear within 21 days of arrival.
- Preparing isolation facilities and reference laboratories should they be needed.
Prevention and Self-Protection
For the general public — especially those planning to travel to affected areas or working in healthcare — the key preventive measures include:
- Avoid travel to areas with active transmission unless truly necessary.
- Avoid contact with the blood and bodily fluids of sick people, and with bodies that have not been handled safely.
- Practice consistent hand hygiene with soap or an alcohol-based sanitizer.
- For health workers: strictly follow infection prevention and control (IPC) protocols and the correct use of personal protective equipment (PPE).
- Be alert to, and do not spread, misinformation; rely only on official sources such as the WHO and national health authorities.
Frequently Asked Questions (FAQ)
Has Bundibugyo Ebola spread beyond Africa? As of this writing, transmission is concentrated in the DRC and Uganda, with two imported cases in Uganda and isolated medically evacuated cases (such as one transferred to Germany). There is no widespread transmission outside the region. See the WHO situation page for DRC 2026 for updates.
Is there an Ebola vaccine? There is a vaccine for the Zaire ebolavirus, but there is no approved vaccine or specific treatment for the Bundibugyo strain causing the 2026 outbreak.
Is Ebola airborne? No. Ebola spreads through direct contact with an infected person’s bodily fluids or contaminated surfaces — not through the air.
What is the fatality rate of Bundibugyo Ebola? In previous BVD outbreaks (2007 and 2012), the CFR ranged from 30% to 50%. In the 2026 outbreak, the early CFR among confirmed cases was around 12%, though this figure may change as the outbreak develops.
Conclusion
The 2026 Bundibugyo Ebola outbreak is a reminder that the threat of infectious disease knows no borders. While the global risk is currently low, vigilance and health literacy remain essential. The combination of a strain with no vaccine, limited diagnostic tools, and an armed conflict at the outbreak site makes this one of the most difficult global health challenges of the year.